Nursing Note Samples
-
Nursing Admission Note
download now -
Nursing Behavior Note
download now -
Nursing Death Note
download now -
Nursing Event Note
download now -
Nursing School Notes Template
download now -
Pediatric Handwritten Nursing Note
download now -

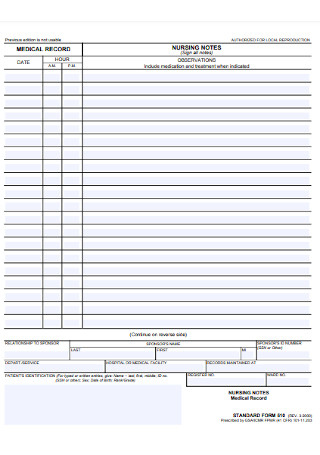
Printable Patient Nursing Notes
download now -
Pharmacology Nursing Care Documentation Note
download now -
Mental Health Charts for Nursing Note
download now -

Vital Soap Notes for Nurses
download now -

Sample Hospital Notes from the Nurse
download now -

Daily Nursing Lecture Notes
download now -
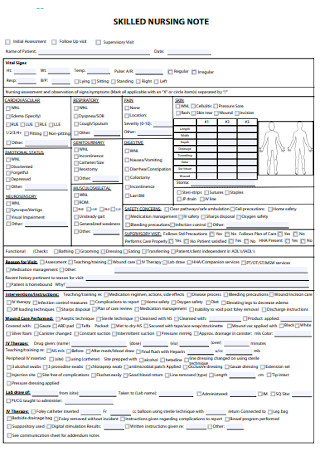
Sample Anatomy Skilled Nursing Note
download now -

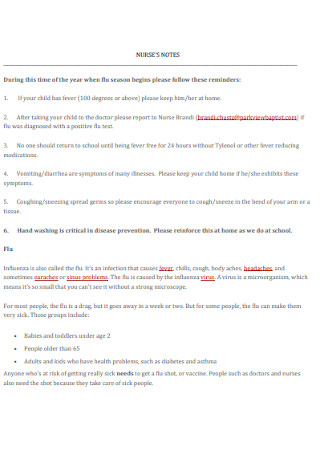
School Nurse Note Cheat Sheet
download now -

Nursing Note Narrative Format
download now -

Nursing Psychiatric Research Note
download now -
Physical Assessment Nursing Medical Note
download now -
Simple Aesthetic Nursing Note
download now -

Nursing Discharge Progress Note
download now -

Nurses Assessment Wound Dressing Note
download now
FREE Nursing Note s to Download
Nursing Note Format
Nursing Note Samples
What is a Nursing Note?
Important Records in a Nursing Note
How to Make Nursing Notes
FAQs
What are the top three important questions to answer in nursing notes?
What are some common labels to write under nursing notes?
What should you not include in nursing notes?
How often should nursing notes be written?
What are common errors to avoid in nursing notes?
Can nursing notes be used in legal cases?
How do nursing notes contribute to patient safety?
Nursing Note Format
Patient Information
- Name: [Patient Name]
- Age: [Age]
- Gender: [Gender]
- Room Number: [Room or Bed Number]
- Date/Time: [MM/DD/YYYY – HH:MM AM/PM]
Subjective Data (What the patient says)
- Chief Complaint: [Patient’s main concern or issue in their own words]
- History of Present Illness (HPI): [Details about the onset, duration, and nature of the current condition]
- Other Patient Statements: [Additional subjective observations or comments from the patient]
Objective Data (What the nurse observes)
- Vital Signs:
- Blood Pressure (BP): [Value]
- Heart Rate (HR): [Value]
- Respiratory Rate (RR): [Value]
- Temperature (Temp): [Value]
- Oxygen Saturation (SpO2): [Value]
- Physical Assessment Findings:
- General Appearance: [Patient’s condition and appearance]
- Neurological: [Alertness, orientation, etc.]
- Cardiovascular: [Heart rate, rhythm, etc.]
- Respiratory: [Breathing effort, lung sounds, etc.]
- Gastrointestinal: [Abdomen findings, bowel sounds, etc.]
- Musculoskeletal: [Mobility, strength, etc.]
Assessment
- Clinical Impression: [Nurse’s analysis based on subjective and objective data]
- Patient Needs: [Identify immediate care priorities]
Plan/Interventions
- Nursing Actions Taken:
- [Medications Administered and Dosage]
- [Interventions Provided, such as wound care or assistance with mobility]
- [Patient Education Given, such as discharge instructions or medication information]
- Physician Notified: [Yes/No, and time of notification if applicable]
- Patient’s Response: [How the patient responded to the interventions or education]
Evaluation
- Patient Progress: [How the patient’s condition has changed, improved, or worsened]
- Follow-Up Needs: [Any pending tasks or observations required for continued care]
Sign-Off
- Nurse’s Name and Designation: [Full Name, RN/LPN, etc.]
- Signature: [Nurse’s Signature]
- Date and Time: [MM/DD/YYYY – HH:MM AM/PM]
What is a Nursing Note?
A nursing note is a formal record created by nurses to document patient care. These notes include observations, assessments, interventions, and patient responses during treatment. Nurses use this documentation to ensure that the patient care plan is carried out effectively and that other healthcare providers have access to detailed information about the patient’s condition. Nursing notes are critical for communication, continuity of care, and maintaining legal and professional standards in nursing practice. You can also see more on File Note.
Important Records in a Nursing Note
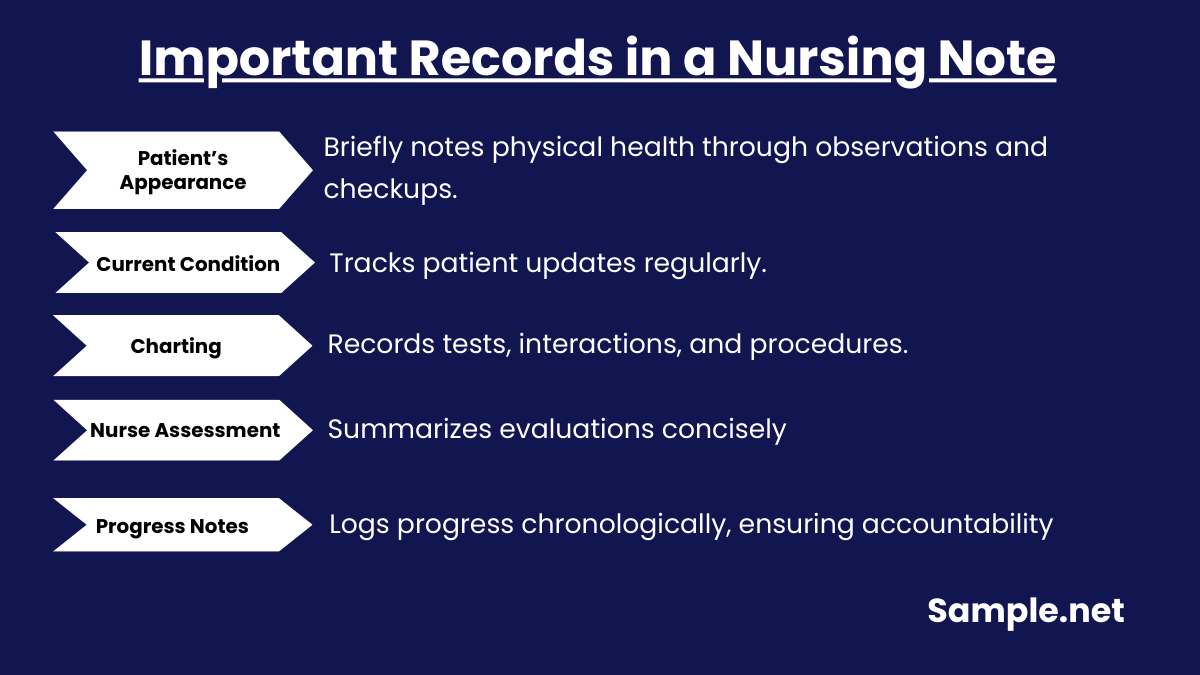
Yes, it is clear that nurses write essential information about their patients and what services were provided under nursing notes. But what exactly can be found inside such notes? In this section, identify the common important records found in nursing notes.
How to Make Nursing Notes
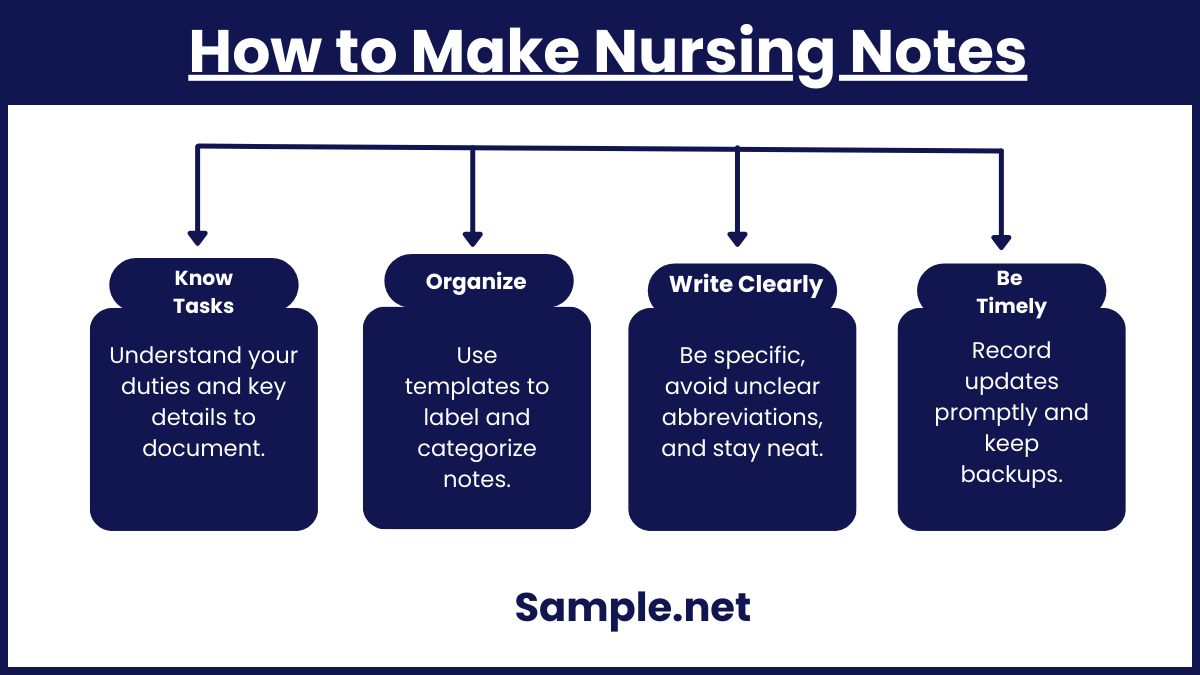
Using the sample nursing notes listed above, you won’t need to start from the very beginning in creating nursing notes. Just use the sample to edit your content, download it anytime, and print as many times as you want. Easy-to-use and customizable templates make it worth your time for sure. You can also see more on Delivery Note. And to ensure you cover everything right, follow these important steps as well:
Step 1: Know Your Tasks and What to Cover
As a nurse, what would be your duties? And what should you cover under your notes? Finalize your roles and tasks to be sure of what to input in the notes. Instructions may differ from one hospital to another. But the common denominator is that you will really cover those important records in a nursing note, which were already discussed earlier. Your purpose will promise you to be guided on what to write along the way.
Step 2: Insert Relevant Labels and Categories into a Template
Labeling and categorizing notes is part of the process, especially when charting is one of the main concerns there. So using a sample template, slowly insert the needed labels and groups for the nursing note. You could tackle head-to-toe examination, wound checkups, late entry records, patient information, health assessment, deceased or not, and so much more.
Step 3: Write Neatly and Specifically
How you write also affects the results. The key is to be very specific with your words and write neatly in the document. That means you avoid abbreviations that may mean different things from other perspectives. And you organize your data promptly so you won’t get confused in following the whole note’s content. Rest assured, your writing slowly improves as you practice note-taking from time to time. You can also see more on Concept Note.
Step 4: Be Timely in Note-Taking
Monitoring a patient’s health requires regular note-taking. So be sure to supervise timely and record essential findings every hour, if you can. Otherwise, your evaluation might fail if there were important points that have not been recorded due to how your details are already outdated. And most importantly, keep extra copies of your notes in case they get lost. Thus, you are still covered with the data from the extra notes.
Nursing notes are indispensable in healthcare, ensuring accurate documentation and effective communication. They enhance patient safety, guide treatments, and provide critical legal and medical records. Comprehensive and precise nursing notes are a cornerstone of quality patient care, reflecting the professionalism and accountability of healthcare providers. You can also see more on Meeting Note.
FAQs
What are the top three important questions to answer in nursing notes?
For your nursing note, be sure to answer the following set of questions:
- Will this data help the rest of the staff who worked with the patient?
- Did the data sum up the patient’s experience?
- Would this data remind me of the patient’s health condition and service about how many years from now, in case you testify on this particular case?
What are some common labels to write under nursing notes?
In writing nursing notes, you are expected to write about the date, patient’s name, nurse’s name, the purpose of visit, appearance, vital signs, patient assessment, diagnostics or lab tests, evaluation of medical interventions, family interactions, additional instructions, and other observations. You can also see more on Research Note.
What should you not include in nursing notes?
Although nursing notes need to be detailed, there is no need to include the patient’s family members’ or friends’ personal details, random abbreviations, dialogues between the provider and the patient, negativity about the staff, and personal opinions.
How often should nursing notes be written?
Nursing notes should be updated in real-time or immediately after patient interactions to maintain accuracy and timeliness in documentation. You can also see more on Thank You Notes.
What are common errors to avoid in nursing notes?
Avoid vague terms, incomplete information, and personal opinions. Always use professional language, be precise, and double-check for accuracy and legibility.
Can nursing notes be used in legal cases?
Yes, nursing notes are legal documents. They can be used as evidence in malpractice cases, audits, or disputes to demonstrate the care provided and adherence to protocols.
How do nursing notes contribute to patient safety?
Nursing notes document critical details like medication administration, changes in condition, and interventions. This ensures accurate communication, preventing errors and enhancing patient safety. You can also see more on Nursing Notes.